I am a neuroscientist and a science blogger. I summarize articles so that you can get the gist of it in less than a minute. I am writing the synopsis in such a way that both non-professional and professional readers can benefit. Every now and then I will feature an older paper, for who among us has read them all? Many studies are from neuroscience and psychology, but definitely not all. Sometimes I post a geeky quote or joke. Happy reading!
A principal investigator tells a graduate student to discover new antibiotics using well known methods. Student discovers new antibiotic. Then, another graduate student performs the antibiotic tests to see if it works. Who takes the credit? The PI got the credit and the Nobel and the money. The discoverer sued and got some credit and some money. The tester got nothing. The tester was a woman. According to the woman’s daughter, “her mother’s colleagues told her it wasn’t important that her name be on the patent because she would one day get married and have a family”.
After the streptomycin controversy, the universities put forth regulations to make (somewhat) clearer who gets what in the process of discovery. Thanks to this and thanks to the women’s liberation movement and, more recently, the women’s fight for equality in workplaces, if this would happen today in a serious University, probably all three would share the Nobel. Probably.
2) Eveleigh, Douglas E.; Bennett, Joan W. (2018-05-01), Whitaker; Barton (eds.), “Women Microbiologists at Rutgers in the Early Golden Age of Antibiotics”,Women in Microbiology, American Society of Microbiology, pp. 317–329, doi:10.1128/9781555819545.ch34, ISBN 978-1-55581-953-8
3) Kingston W (July 2004). “Streptomycin, Schatz v. Waksman, and the balance of credit for discovery”. Journal of the History of Medicine and Allied Sciences. 59 (3): 441–462. doi: 10.1093/jhmas/jrh091. PMID 15270337. S2CID 27465970.
Few of the Generation X people are unfamiliar with the super-hit/movie cult Twin Peaks. And from those, even fewer find the dwarf dancing in the Red Room not scary as hell. And yet even fewer know who the man singing “Sycamore Trees” in that room is. For memory refreshment, here is the clip.
The man with the unusual voice, to match all the rest of the… um… “unusualness”, is none other than Jimmy Scott, a phenomenal jazz singer. If you listen to him, particularly in the hit “I’m Afraid The Masquerade Is Over“, you’ll notice that, if you close your eyes, you might be confused on whether the voice belongs to an adult man or a very gifted prepubertal boy.
And that is because Jimmy Scott suffered his entire life from a rare and obscure disease, called the “Kallmann syndrome”. This is a genetic disorder that prevents a person to start or to fully complete puberty. And that is because they have low circulating sex hormones: testosterone in males and estrogen and progesterone in females. And that is because their hypothalamus does not produce enough or at the proper times gonadotropin-releasing hormone (GnRH). And that is because sometime during the first trimester of pregnancy, there was an abnormality in the development of the olfactory fibers. You might ask what does smell development has with sex hormones? Well, I’m glad you asked. The cells that will end up releasing GnRH during puberty need to migrate from where they are born (nasal epithelium) to hypothalamus. If something impedes said migration, like, say, a mass, then the cells cannot reach their destination and you get a person who cannot start or finish puberty, plus a few other symptoms (Teixeira et al., 2010).
As some of you might have already surmised, something else besides lack of puberty must happen to these people regarding their sense of smell. After all, their olfactory fibers got tangled during embryonic development, forming, probably, a benign tumor, a neuroma. Not surprisingly, the person ends up with severely diminished or absent sense of smell, information that can be clinically used for diagnosis (Yu et al., 2022).
The first one to notice that people with failure to start or fully complete puberty are also anosmic was Aureliano Maestre de San Juan, a Spanish scientist. Unfortunately, the syndrome he documented in 1856 was named not named after him, but after the German scientist Franz Joseph Kallmann who described it almost a century later, in 1944 (Martin et al., 2011). Kallmann not only he did not discover the syndrome himself, but he was a staunch supporter of “racial hygiene”, advocating for finding and sterilizing relatives of people with schizophrenia so to eradicate the disease from future generations. Ironically, he fled Germany in 1939 because he was of Jewish heritage into a country which enthusiastically embraced eugenics and performed their own sterilizations programs, the USA (Benbassat, 2016).
So, I hereby propose, in an obscure unvisited corner of the Internet, to rename the disease the Maestre syndrome or MSJJ, after the guy who actually noticed it the first time and published about it. Besides, it’s his birthday today, having been born on October 17, 1828.
Original references which I couldn’t find, as they appear in Martin et al. (2011):
Maestre de San Juan A. (1856). Teratologia: Falta total de los nervios olfactorios con anosmia en un individuo en quien existia una atrofia congénita de los testículos y miembro viril. Siglo Medico, 3:211–221 [Google Scholar]
Kallmann F, Schoenfeld W & Barrera S (1944). The genetic aspects of primary eunuchoidism. Am J Ment Defic, 48:203–236 [Google Scholar]
I want to share an observation that’s been on my mind for a while. I was visiting a Zoo with my family before the vaccine was available for regular people, around early Spring 2021. A big Zoo. All the enclosures where animals were indoors (penguins, monkeys and so on) had a big sticker on the door asking to “Please wear a mask for our animals’ sake. They too can get COVID19”. An overwhelming majority were putting on their masks upon reading this sign. Really, close to 99% of people, adults and children alike. At the same zoo, the same people were entering maskless in the Gift Shop and other indoor facilities like toilets and so on. I eyeballed less than 10% were wearing masks in “human enclosures”. I spent a lot of time at this Zoo watching for this behavior instead of looking at the other animals to make sure I’m not imagining things.
My lesson: humans are not deemed worthy the masking trouble, but zoo animals are… Now please explain to me how no mask-wearing is about “freedom”, “COVID is a scam/flu/doesn’t exist”, “masks don’t work” and so on and not about a conscious moral choice to knowingly endanger other people and their kids?
By Neuronicus, 17 August 2021
EDIT: Mrs. Clinton’s first name is Hillary, not Hilary.
REFERENCES:
Howard J, Huang A, Li Z, Tufekci Z, Zdimal V, van der Westhuizen HM, von Delft A, Price A, Fridman L, Tang LH, Tang V, Watson GL, Bax CE, Shaikh R, Questier F, Hernandez D, Chu LF, Ramirez CM, Rimoin AW. (26 Jan 2021). An evidence review of face masks against COVID-19.Proceeding of the National Academy of Sciences of the USA, 118(4):e2014564118. doi: 10.1073/pnas.2014564118. PMID: 33431650. ARTICLE| FREE FULLTEXT PDFP.S. Since this paper was published, dozens of others have been published that say the same thing: wear a mask for all our sakes.
The authors used a chemical transport model called GEOS-Chem to estimate the global exposure levels to airborne particulate matter derived from fossil fuel combustion. It’s a worldwide used model for estimating dispersion, for example the simulation of surface pollination. The model has been validated, meaning its predictions were compared with the reality and they matched. Levels of fossil fuels emission were inputted from publicly available data “from multiple sectors (power generation, industry, ships, aircraft, ground transportation, backup generators, kerosene, oil/gas extraction), detailed oxidant-aerosol chemistry, and reanalysis meteorology from the NASA Global Modeling and Assimilation Office” (page 5 of the manuscript). The mortality due to air pollution was computed by starting with the classical risk assessment analysis from epidemiological research and then adjusting for other variables like in-door particulate exposure (smoking) and so on. It sounds straightforward enough but the math and stats involved are very complicated. You have to take into consideration concentration, exposure time, and other factors that affect the outcome.
In addition, the authors calculated the mortality caused by fossil-fuel air pollution in children between 0 and 4 years of age, which was 876 in North America, 747 in South America, and 605 in Europe, annually. Pollution data is from 2012, mortality from 2015. The authors are hopeful that aggressive regulation designed to curb emissions in the last few years may have already lowered these numbers. Policy-makers, take note!
I re-blog other people’s posts extremely rarely. But this one is worth it. It’s about how groups form based on the amount of information given. And, crucially, how amount of information can change individual behavior and group splits. It relates to political polarization and echo-chambers. Read it.
After you read it, you will understand my following question: I wonder by how much the k would increase in a non-binary environment, say the participants are given 3 colors instead of 2. The authors argue that there is a k threshold after which the amount of information makes no difference any more. But that is because the groups already completed the binary task, therefore more information is useless due to the ceiling effect. Basically, my question is: at which point more information stops making a difference in behavior if there were more choices? Is it a log scale, linear, exponential? Good paper, good cover by CNRS, at scienceblog.
By Neuronicus, 24 February 2021
P.S. I haven’t written in a while due to many reasons, one of which is this pesky WordPress changed the post Editor and frankly I don’t have the time and patience to figure it out right now. But I’ll be back :).
L is for length and W is for… circumference. I could have corrected the pic, but it generated far more interesting comments as it is on social media.
REFERENCE: Veale D, Miles S, Bramley S, Muir G., & Hodsoll J (Jun 2015). Am I normal? A systematic review and construction of nomograms for flaccid and erect penis length and circumference in up to 15 521 men. British Journal of Urology International, 115(6):978-986. PMID: 25487360, DOI: 10.1111/bju.13010. ARTICLE|FREE FULLTEXT PDF|Editorial|Science cover
Some meme is circulating around saying that for any 1 dead of COVID-19 there is an x amount of people who survive but experience vastly debilitating and sometimes life long lasting diseases. That x number is usually a subject of controversy based on little or confusing hearsay-type of information. The believers in the x number use it to argue that mask-wearing and healthier behaviors literally save lives of people, while the non-believers in the x number, well… they just don’t believe the x number exists at all and that’s that. Either you die of COVID-19 or you survive and make a full recovery. I prefer to think that this is the case instead of the unfortunately way more probable, callous, cruel and dehumanizing “x exists and so what, I’m ok with people dying, ‘cause people die all the time, as long as it’s not me”.
The x number exists all right. Paterson et al. (2020) just published a paper last week (July 8th) that puts some numbers in the place of x, at least when it concerns neurological disorders. Because I have heard all sorts of “excuses” like, yeah, but those people who had it bad were old, had previous medical conditions, were black or poor or [insert your favorite post-hoc rationalization here], I decided to comb through the paper’s supplementals and give you a bit more of the background of the people investigated in this article.
If you’re not interested, you can skip the following section and go directly to the conclusion as long as you get the take-home message: many people of all sorts of ages and races, with no previous medical conditions and with mild COVID-19 symptoms can still have life long seriously debilitating neurological conditions. How many, you ask? I’m eyeballing almost a half of the investigated patients in this paper were not “at risk” in any way.
So. We have 43 patients treated from April 9 to May 15, 2020, in UK, out of which:
29 were SARS-CoV-2 PCR positive and definite, meaning a PCR test.
8 were probable meaning “clinical and laboratory features highly suggestive of COVID-19—lymphopenia, raised D-dimer, suggestive chest radiology in the absence of PCR evidence” p. 6
6 were possible in whom “temporal or laboratory features indicate an association but another cause was also found” p. 6
Demographics: 24 males and 19 females with ages ranging from 16–85 years, 53% were non-white.
Symptoms were classified as:
Mild (non-pneumonia or mild pneumonia)
Severe (dyspnoea and hypoxia requiring supplementary oxygen)
Both females and males, both whites and non-whites
Hospital admission reason: 6 neurological, 1 respiratory, 3 both
Past medical history : 4 none, 3 hypertension, 2 cancer, 1 stroke, 2 diabetes, 1 asthma
Days of onset of encephalopathies from onset of COVID-19 symptoms: -4 to 21
Severity of COVID-19 symptoms: 6 mild, 2 severe, 2 critical
Diagnosis: 8 definite, 2 probable COVID-19
Recovery: 7 complete, 1 incomplete, 1 significant, 1 not recovered.
Survival: all 10 are alive
Vignette A: As a note for people who think a bit of delirium is not a big deal, let’s peak at a case that the authors describe in the paper for representative reasons. A 55-year old White woman with no previous medical or psychiatric conditions was admitted to hospital with mild to severe COVID-19 symptoms and a positive SARS-CoV2 test. She stayed in the hospital for 3 days, requiring minimal oxygen. But after discharge, the woman started behaving oddly, confused, agitated, putting on and off her coat repeatedly, hallucinated lions and monkeys in the house, other auditory hallucinations, had persecutory delusion, Capgras delusion (husband replaced by impostor), and became aggressive and combative with family and hospital staff. This started 17 days after her fist COVID-19 symptoms which were fever, cough, aches and loss of smell and taste. Normal brain MRI and EEG. She was put on serious antipsychotics with an on-off improvement result. She’s classified as significantly recovered.
12 patients had neuroinflammatory syndromes (encephalitis) post-COVID
Age: 27-60
Hospital admission reason: 6 neurological, 1 respiratory, 3 both
Both females and males, both whites and non-whites
Days of onset of syndrome from onset of COVID-19 symptoms: -6 to 27
Severity of COVID-19 symptoms: 6 mild, 2 severe, 2 critical
Diagnosis: 8 definite, 3 probable, 1 possible
Past medical history: 3 none, 3 diabetes, 2 asthma, 3 hypertension, 2 arthritis, 1 hypothyroidism, 1 treated breast cancer with high cholesterol and other diseases and this is the one who died.
Severity of COVID-19 symptoms: 6 mild, 2 severe, 4 critical
Recovery: 1 complete, 10 incomplete, 1 died
Survival: 11 alive, 1 dead (which had mild symptoms)
Vignette B: A 65-year-old Black female with osteoarthritis and a 2-year history of cognitive decline was admitted for involuntary right hand and then widespread involuntary movements. Then she developed complex visual hallucinations (people in the house, objects flying in the room), vision impairments including double vision, speaking impairments, disorientation and confusion, shaking, remarkable twitching and hyper reflexes. “MRI brain, EEG and CSF examination were normal” p. 12. She had a positive SARS-CoV2 test and severe COVID-19 symptoms, meaning she required oxygen therapy. Given medicines for muscle spasms and oxygen for COVID-19. She’s classified as incomplete recovery.
Vignette C: A 52-year-old Asian male with asthma presented with 10 days of cough, difficulty breathing and muscle aches. The SARS-CoV2 test was positive. His oxygen supply was getting worse and he required intubation for 17 days, meaning now his symptoms are considered critical. He was slow to wake up from intubation. MRI showed significant lesions and cysts with white matter damage and haemorrhage. He has a severely impaired conscious level responding to pain only. He’s classified as incomplete recovery.
Vignette D: A 47 year old female of Other ethnicity with asthma as a previous medical condition presented neurological symptoms: left side numbness and weakness, with headache, vomiting and reduced conscious level. Prior to this, for a week she had cough, fever and shortness of breath. All other markers and symptoms (minus neurological) pointed to COVID-19 but no PCR test was administered. Because she had low conscious level she was incubated, thus her COVID-19 symptoms are catalogued as severe, even if the reason of intubation was not low oxygen. MRI showed severe brain and brain blood vessels swelling. Was aggressively treated for brain swelling. After 2 days of this treatment when she was not responding and when she developed fixed dilated right pupil, emergency surgery was performed to remove part of her skull to release intracranial pressure from all the swelling. After 4 more days of intubation she was de-intubated and “continues to improve clinically, and is able to weight bear with support” p. 10. She’s classified as incomplete recovery.
Vignette E: A 52 year-old White male with no past medical history presented with progressive limb weakness, headache, vomiting, and back pain that lasted for the past 3 days. MRI showed multiple lesions in the brain. Over 5 days, these lesions increased in size and there were multiple bleeding sites in the brain. He was positive for SARS-CoV2 and 3 days later developed fever and shortness of breath. About the same time his neurological symptoms increased in severity and number. A nerve conduction test supported a diagnosis of Guillain–Barré syndrome (a nasty autoimmune disease in which your immune system eats your nerves). He was intubated due to oxygen requirements. Three days after corticosteroid treatment he was able to open eyes and mouth words and after 2 weeks, he was able to talk and flex both arms. He’s classified as incomplete recovery. He’s still in the hospital.
8 patients had strokes post-COVID
Age: 24 -85
Both females and males, both whites and non-whites.
Days of onset of syndrome from onset of COVID-19 symptoms: -2 to 15.
Severity of COVID-19 symptoms: 6 mild, 2 severe, 2 critical
Diagnosis: 6 definite, 2 probable
Reason for hospital admission: 5 neurological, 3 respiratory
Past medical history: 2 none, 2 with hypertension, 1 with stroke, 1 obese, 2 heart disease (1 of them is the one who died) and others
Severity of COVID-19 symptoms: 5 mild, 3 severe
Recovery: 1 complete, 3 incomplete, 1 no improvement (3 still in the hospital)
Survival: 7 alive, 1 dead (of the ones with severe symptoms)
Vignette F: A 58-year-old Black male with only arthritis of the spine as a pre-existing condition came to the hospital with difficulty in speaking and weakness on the right side after 2 days of coughing and being tired. He had a high-risk occupation for getting COVID-19 and all other COVID-19 signs and symptoms were there minus a COVID-19 test. So he is thought to be probably carrying it. Brain CT showed a stroke. Treated with heparin for a lung blood clot and other anti-blood clot medicines for the stroke. On day 8 he was discharged to the Rehabilitation unit of the hospital.
7 patients developed Guillain–Barré syndrome (GBS) post-COVID
Age: 20-63
All males, both whites and non-whites.
Days of onset of syndrome from onset of COVID-19 symptoms: -1 to 21.
Severity of COVID-19 symptoms: 6 mild, 2 severe, 2 critical
Diagnosis: 4 definite, 4 possible
Reason for hospital admission: all neurological
Past medical history: 4 none, 1 with stroke and myeloma, 1 with high cholesterol, and 1 with diabetes, headaches and arrhythmia
Severity of COVID-19 symptoms: 7 mild, 1 severe
After treatment with immunoglobulins: 1 requires assisted ventilation, 1 is bedridden, 5 able to walk 5m but incapable of manual work/running, and 1 unknown
Survival: all
5 patients developed neurological symptoms difficult to characterizepost-COVID
Age: 16-40
Both males and females, both whites and non-whites.
Days of onset of syndrome from onset of COVID-19 symptoms: 6 to 26.
Severity of COVID-19 symptoms: 2 mild, 1 severe, 2 critical
Diagnosis: 3 definite, 1 probable, 1 possible
Reason for hospital admission: 2 neurological, 2 respiratory, 1 other
Past medical history: 1 none, 1 heavy periods, 1 with epilepsy, hypertension, congenital disorders and all sorts of other stuff, 1 with leukemia, and 1 with inflammation of the eyes and joints
Severity of COVID-19 symptoms: 7 mild, 1 severe
Recovery: 1 complete, 3 incomplete , and 1 no improvement (3 still in the hospital)
Survival: 7 alive, 1 dead (of the ones with severe symptoms)
These patients’ symptoms ranged from the headaches to seizures, from weakness to low conscious level. Some also had hemorrhages, encephalopathy, brain abscess, diarrhea, cardiac stuff, all sorts. MRIs were all abnormal except for the one who was declared recovered and discharged.
CONCLUSIONS
To recapitulate, what I did was basically re-write the paper’s tables in lay terms because few of us are proficient in medical jargon, but, more importantly, even fewer – except the scientists and medical doctors – have the time and patience to comb through the supplemental to form the image I gave you. So here you go. Professionals don’t need my blog, they can go directly to the bottom of the post and read the source in original. The image I wanted to convey is that
By long lasting I mean “irreversible”, even if slowly improvable. Please note that the vast majority of these patients were admitted to the hospital not for COVID-19 respiratory symptoms, but for neurological symptoms.
There’s also something else of extraordinary interest in the paper. Eight of the patients had either brain biopsies or spinal tap tested for SARS-CoV2 and all these tests were negative, meaning the virus is not itself causing these neurological problems. In some patients, there was evidence of the cytokine storm, meaning the virus put the immune system in overdrive and this one, in turn, attacked the body, here the brain. So far, the autoimmune hypothesis seems to be the most plausible and parsimonious explanation.
As far the x number is concerned, the authors just gave us the data and let us interpret it. They do offer a hint of just how to interpret them though: the number of brain inflammation cases they saw in 5-weeks is normally seen in London only over a period of 5 months (p. 14). You do the math.
Also, some commentator on the Facebook post raised the question of asymptomatics. Which is a very good question. How do they fare? I don’t know and neither are you. But let me remind you that most of the people in this study were admitted to hospital for neurological reasons, not COVID-19 symptoms. So if they were never having the COVID-19 symptoms, i.e. were asymptomatics, nobody would have done a COVID-19 test on them… and so they’d be treated as regular neurological patients. To figure out what happens to the asymptomatics we need to wait probably a year when we can look at the general epidemiological incidence of heart attacks or GBS or strokes in the general population. And so we’ll probably attribute that increase to COVID-19.
REFERENCE: Paterson RW, Brown RL, Benjamin L, Nortley R, Wiethoff S, Bharucha T, Jayaseelan DL, Kumar G, Raftopoulos RE, Zambreanu L, Vivekanandam V, Khoo A, Geraldes R, Chinthapalli K, Boyd E, Tuzlali H, Price G, Christofi G, Morrow J, McNamara P, McLoughlin B, Lim ST, Mehta PR, Levee V, Keddie S, Yong W, Trip SA, Foulkes AJM, Hotton G, Miller TD, Everitt AD, Carswell C, Davies NWS, Yoong M, Attwell D, Sreedharan J, Silber E, Schott JM, Chandratheva A, Perry RJ, Simister R, Checkley A, Longley N, Farmer SF, Carletti F, Houlihan C, Thom M, Lunn MP, Spillane J, Howard R, Vincent A, Werring DJ, Hoskote C, Jäger HR, Manji H, Zandi MS; UCL Queen Square National Hospital for Neurology and Neurosurgery COVID-19 Study Group (8 Jul 2020). The emerging spectrum of COVID-19 neurology: clinical, radiological and laboratory findings, Brain, online ahead of print PMID: 32637987. DOI: 10.1093/brain/awaa240ARTICLE | FREE FULLTEXT PDF | SUPPLEMENTALS | Deutsche Welle cover | University College London Press release
There is hope for a vaccine. Serious hope. It will take probably 12 to 18 months until we have it. Maybe a little bit longer. But it looks like we will have it. Just continue your physical distancing, wear masks, be considerate to your fellow humans and it’ll be alright. We’ll bounce back and because we – the people – make up this extraordinary concept of economy, so shall it. After this pandemic will pass, hopefully we will not return to normal; instead, we will emerge a bit wiser, a bit more careful, a bit more compassionate. Meanwhile, throw some grateful words to your nearest scientist, whether or not they work on COVID-19.
REFERENCE: Callaway, E. (28 April 2020). The race for coronavirus vaccines: a graphical guide,Nature, 580: 576-577 (2020). doi: 10.1038/d41586-020-0121-y. FREE FULLTEXT PDF
In the past few days, a new hot subject has gripped the attention of various media and concerned the medical doctors, as if they don’t have enough to deal with: chloroquine. That is because the President of the U.S.A., Donald Trump, endorsed chloroquine as treatment of COVID-19, a “game changer”, despite his very own director of the National Institute of Allergy and Infectious Diseases (NIAID), Dr. Anthony Fauci, very emphatically and vehemently denying that the promise of (hydroxy)chloroquine is beyond anecdotal (see the White House briefing transcript here).
Many medical doctors spoke out urging caution against the drug, particularly against the combination the President endorses: hydroxychloroquine + azithromycin. As I understand it, this combo can be lethal as it can lead to fatal arrhythmia.
As for the (hydroxy)cloroquine’s possibility to help treat COVID-19, the jury is still out. Far out. Meaning that there have been a few interesting observations of the drugs working in a Petri dish (Liu et al. 2020, Wang et al., 2020), but as any pharma company knows, there is a long and perilous way from Petri dishes to pharmacies. To be precise, only 1 in 5000 drugs get from pre-clinical trials to approval and it takes about 12 years for this process to be completed (Kaljevic et al., 2004). The time is so long not because red tape, as some would deplore, but because it takes time to see what it does in humans (Phase 0), what doses are safe and don’t kill you (Phase 1), does it work at all for the intended disease (Phase 2), compare it with other drugs and evaluate the long-term side effects (Phase 3) and, finally, to see the risks and benefits of this drug (Phase 4). While we could probably get rid of Phase 0 and 4 when there is such a pandemic, there is no way I would submit my family to anything that hasn’t passed phases 1, 2, and 3. And those take years. With all the money that a nation-state has, it would still take 18 months to do it semi-properly.
Luckily for all of us, chloroquine is a very old and established anti-malarial medicine, and as such we can safely dispense of Phases 0, 1, and 4, which is fine. So we can start Phase 2 with (hydroxy)chloroquine. And that is exactly what WHO and several others are doing right now. But we don’t have enough data. We haven’t done it yet. So one can hope as much as they want, but that doesn’t make it faster.
Unfortunately – and here we go to the crux of the post -, following the President’s endorsement, many started to hoard chloroquine. Particularly the rich who can afford to “convince” an MD to write them a script for it. In countries where chloroquine is sold without prescription, like Nigeria, where it is used for arthritis, people rushed to clear the pharmacies and some didn’t just stockpiled it, but they took it without reason and without knowing the dosage. And they died. [EDIT, 23 March 2020. If you think that wouldn’t ever happen in the land of the brave, think again, as the first death to irresponsible taking chloroquine just happened in the USA]. In addition, the chloroquine hoarding in US by those who can afford it (is about $200 for 50 pills) lead to lack of supply for those who really need it, like lupus or rheumatology patients.
For those who blindly hoard or take chloroquine without prescription, I have a little morsel of knowledge to impart. Remember I am not an MD; I hold a PhD in neuroscience. So I’ll tell you what my field knows about chloroquine.
Both chloroquine and hydroxychloroquine can cause severe psychosis.
That’s right. More than 7.1 % of people who took chloroquine as prophylaxis or for treatment of malaria developed “mental and neurological manifestations” (Bitta et al., 2017). “Hydroxychloroquine was associated with the highest prevalence of mental neurological manifestations” (p. 12). The phenomenon is well-reported, actually having its own syndrome name: “chloroquine-induced psychosis”. It was observed more than 50 years ago, in 1962 (Mustakallio et al., 1962). The mechanisms are unclear, with several hypotheses being put forward, like the drugs disrupting the NMDA transmission, calcium homeostasis, vacuole exocytosis or some other mysterious immune or transport-related mechanism. Because the symptoms are so acute, so persistent and so diverse than more than one brain neurotransmitter system must be affected.
Chloroquine-induced psychosis has sudden onset, within 1-2 days of ingestion. The syndrome presents with paranoid ideation, persecutory delusions, hallucinations, fear, confusion, delirium, altered mood, personality changes, irritability, insomnia, suicidal ideation, and violence (Biswas et al., 2014, Mascolo et al., 2018). All these at moderately low or therapeutically recommended doses (Good et al., 1982). One or two pills can be lethal in toddlers (Smith & Klein-Schwartz, 2005). The symptoms persist long after the drug ingestion has stopped (Maxwell et al., 2015).
Still want to take it “just in case”?
P.S. A clarification: the chemical difference between hydroxychloroquine and chloroquine is only one hydroxyl group (OH). Both are antimalarial and both have been tested in vitro for COVID-19. There are slight differences between them in terms of toxicity, safety and even mechanisms, but for the intents of this post I have treated them as one drug, since both produce psychosis.
REFERENCES:
1) Biswas PS, Sen D, & Majumdar R. (2014, Epub 28 Nov 2013). Psychosis following chloroquine ingestion: a 10-year comparative study from a malaria-hyperendemic district of India.General Hospital Psychiatry, 36(2): 181–186. doi: 10.1016/j.genhosppsych.2013.07.012, PMID: 24290896 ARTICLE
2) Bitta MA, Kariuki SM, Mwita C, Gwer S, Mwai L, & Newton CRJC (2 Jun 2017). Antimalarial drugs and the prevalence of mental and neurological manifestations: A systematic review and meta-analysis. Version 2. Wellcome Open Research, 2(13): 1-20. PMCID: PMC5473418, PMID: 28630942, doi: 10.12688/wellcomeopenres.10658.2 ARTICLE|FREE FULLTEXT PDF
4) Good MI & Shader RI. Lethality and behavioral side effects of chloroquine (1982). Journal of Clinical Psychopharmacology, 2(1): 40–47. doi: 10.1097/00004714-198202000-00005, PMID: 7040501.ARTICLE
3) Kraljevic S, Stambrook PJ, & Pavelic K (Sep 2004). Accelerating drug discovery. EMBO Reports, 5(9): 837–842. doi: 10.1038/sj.embor.7400236, PMID: 15470377, PMCID: PMC1299137. ARTICLE| FREE FULLTEXT PDF
4) Mascolo A, Berrino PM, Gareri P, Castagna A, Capuano A, Manzo C, & Berrino L. (Oct 2018, Epub 9 Jun 2018). Neuropsychiatric clinical manifestations in elderly patients treated with hydroxychloroquine: a review article. Inflammopharmacology, 26(5): 1141-1149. doi: 10.1007/s10787-018-0498-5, PMID: 29948492. ARTICLE
5) Maxwell NM, Nevin RL, Stahl S, Block J, Shugarts S, Wu AH, Dominy S, Solano-Blanco MA, Kappelman-Culver S, Lee-Messer C, Maldonado J, & Maxwell AJ (Jun 2015, Epub 9 Apr 2015). Prolonged neuropsychiatric effects following management of chloroquine intoxication with psychotropic polypharmacy.Clinical Case Reports, 3(6): 379-87. doi: 10.1002/ccr3.238, PMID: 26185633. ARTICLE | FREE FULLTEXT PDF
6) Mustakallio KK, Putkonen T, & Pihkanen TA (1962 Dec 29). Chloroquine psychosis?Lancet, 2(7270): 1387-1388. doi: 10.1016/s0140-6736(62)91067-x, PMID: 13936884. ARTICLE
7) Smith ER & Klein-Schwartz WJ (May 2005). Are 1-2 dangerous? Chloroquine and hydroxychloroquine exposure in toddlers.The Journal of Emergency Medicine, 28(4): 437-443. doi: 10.1016/j.jemermed.2004.12.011, PMID: 15837026. ARTICLE
Studies about chloroquine and hydoxychloroquine on SARS-Cov2 in vitro:
Liu, J., Cao, R., Xu, M., Wang, X., Zhang, H., Li, Y., Hu, Z., Zhong, W., & Wang, M. (18 March 2020). Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discovery, 6 (16), https://doi.org/10.1038/s41421-020-0156-0ARTICLE | FREE FULLTEXT PDF
Wang, M., Cao, R., Zhang, H., Yang, X., Liu, J., Xu, M., Shi, Z., Hu, Z., Zhong, W., & Xiao, G. (18 March 2020). Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Research, 30: 269–271. https://doi.org/10.1038/s41422-020-0282-0.ARTICLE | FREE FULLTEXT PDF
First study about chloroquine and hydoxychloroquine on SARS-Cov2 in vivo below. Unfortunately, it has some methodological flaws, see here and here, which hopefully will be corrected once the peer-reviewers will take a closer look at it. UPDATE [31-3-2020]: It seems the article is flawed in more than one way, with serious ethical issues (timeline of treatment doesn’t match the methods reported, patients appear and disappear from data points, graphs different depending on the venue, published in the same journal where the author is editor, no peer-review, no blind, no placebo, controls barely tested, plus, no reputable researcher should announce that they are the genius that cured COVID-19 on a YouTube video, particularly when they get to publish in 24 hours anyway).
Anyway, here it is:
Gautret P, Lagier J-C, Parola P, Hoang VT, Meddeb L, Mailhe M, Doudier B, Courjon J, Giordanengo V, Esteves Vieira V, Tissot Dupont H,Colson SEP, Chabriere E, La Scola B, Rolain J-M, Brouqui P, Raoult D. (20 March 2020). Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. International Journal of Antimicrobial Agents, PII:S0924-8579(20)30099-6, https://doi.org/10.1016/j.ijantimicag.2020.105949. ARTICLE | FREE FULLTEXT PDF
These studies are also not peer reviewed or at the very least not properly peer reviewed. I say that so as to take them with a grain of salt. Not to criticize in the slightest. Because I do commend the speed with which these were done and published given the pandemic. Bravo to all the authors involved (except maybe the last one f it proves to be fraudulent). And also a thumbs up to the journals which made the data freely available in record time. Unfortunately, from these papers to a treatment we still have a long way to go.
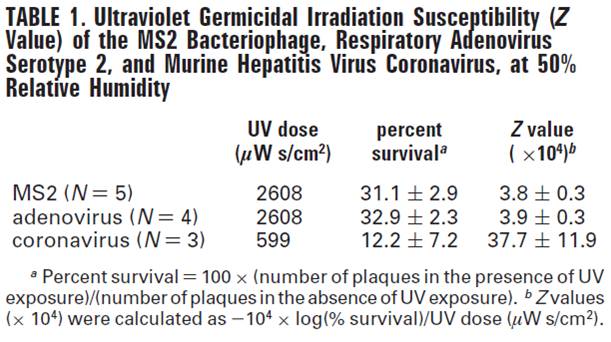
I was looking for what kills coronaviruses and I found this little gem in a paper by Walker & Ko (2007):
“MHV coronavirus was easily inactivated in PBS with 0.01% Tween but was relatively stable when suspended in MEM with 10% FBS”.
Tween is a relatively inexpensive standard molecular biology reagent for cell culture. Is otherwise known as POE (20) sorbitan monooleate, Polyethylene glycol sorbitan monooleate, Polyoxyethylenesorbitan monooleate, Polysorbate 80, Sigma says. It costs about $30 for 100 ml, but you could probably get it cheaper if bought in bulk, like I did a few months ago.
The paper in itself is on a different subject: comparing survival rate of the infectious agents after exposure to UV light. The one sentence about Tween was put in to emphasize differences between the infectious agents. The actual point of the paper is that while the bacteriophage MS2 and the respiratory adenovirus serotype 2 were not affected too much by UV, the murine hepatitis coronavirus was. Namely, after exposure to a dose of 599 microW s/cm2 of 254 nm UV, the coronavirus survival was only 12.2 % +/- 7.2, but to reduce the MS2 and adenovirus survival rate to around 32%, a much higher dose of UV of 2608 microW s/cm2 was needed (see Table).
From Walker & Ko (2007).
The infectious agents were aerosolized. This is important because the “UV susceptibility is higher in viral aerosols than in viral liquid suspensions” (p. 5464).
Of extreme importance: DO NOT SHINE UV ON SKIN! It will harm you more than it will harm the virus:
The only thing I’m a bit unclear is the duration of UV exposure. In the Methods it says: “16.2 s at 12.5 L/min airflow […] was considered the UV exposure time” (p. 5461), but elsewhere in the paper we find: “The duration of sample collection was 15 min, with the UV on (UV dose = 2608 or 599 microWs/cm2) or off” (p. 5462). So weren’t the aerosols exposed for 15 minutes then? Or they passed away since there was an airflow in the experimental chamber and then they were only exposed for 16 sec? I dunno, it’s not my field.
Nor is cell culture my field, so I’m definitely not an expert though I have learned how to do it as a matter of principle because it keeps happening around me and in the papers I read. So perhaps the fact that Tween kills coronaviruses might be common knowledge for a good portion of the molecular biologists and immunologists, but maybe not for everybody. So here you go:
P.S. As soon as I published, I have been thoroughly (and repeatedly!) informed that every scientist that works with viruses knows that Tween kills coronaviruses. Because… drum roll… Tween is a soap. Duh! And we know how soap kills viruses, by dissolving their protective cover. Oh well :). I’d rather be chided for repeating well-known facts than for spreading disinformation.
REFERENCE: Walker, C. M., & Ko, G. (1 Aug 2007). Effect of Ultraviolet Germicidal Irradiation on Viral Aerosols. Environmental Science & Technology, 41(15), 5460–5465. PMID: 17822117, DOI: 10.1021/es070056uARTICLE
After reading these two words, my first thought was that you can have a whole range of people, some compassionate but not polite (ahem, here, I hope), polite but not compassionate (we all know somebody like that, usually a family member or coworker), or compassionate and polite (I wish I was one of those) or neither (some Twitter and Facebook comments and profiles come to mind…).
It turns out that it is not the case. As in: usually, people are either one or another. Of course there are exceptions, but the majority of people that seem to score high on one trait, they tend to score low on the other.
Hirsh et al. (2010) gave a few questionnaires to over 600 mostly White Canadians of varying ages. The questionnaires measured personality, morality, and political preferences.
After regression analyses followed by factor analyses, which are statistical tools fancier than your run-of-the-mill correlation, the authors found out that the polite people tend to be politically conservatives, affirming support for the Canadian or U.S. Republican Parties, whereas the compassionate people more readily identified as liberals, i.e. Democrats.
Previous research has shown that political conservatives value order and traditionalism, in-group loyalty, purity, are resistant to change, and that they readily accept inequality. In contrast, political liberals value fairness, equality, compassion, justice, and are open to change. The findings of this study go well with the previous research because compassion relies on the perception of other’s distress, for which we have a better term called empathy. “Politeness, by contrast, appears to reflect the components of Agreeableness that are more closely linked to norm compliance and traditionalism” (p. 656). So it makes sense that people who are Polite value norm compliance and traditionalism and as such they end up being conservatives whereas people who are Compassionate value empathy and equality more than conformity, so they end up being liberals. Importantly, empathy is a strong predictor for prosocial behavior (see Damon W. & Eisenberg N (Eds.) (2006). Prosocial development, in Handbook of Child Psychology: Social, Emotional, and Personality Development, New York, NY, Wiley Pub.).
I want to stress that this paper was published in 2010, so the research was probably conducted a year or two prior to publication date, just in case you were wondering.
1) an error in judgment, skill, or coordination of care,
2) a diagnostic error,
3) a system defect resulting in death or a failure to rescue a patient from death, or
4) a preventable adverse event.” (Letter to CDC by Makary et al., 2016)
I reproduced the authors’ definition because there is a hot debate in the medicine field as to what constitutes a medical error and what is preventable vs. unpreventable. It might seem clear cut to you and me, but after I perused a few papers from both sides I must admit that things seem (a bit) more complicated than I thought. Personally, I’m all onboard with the above definition.
Also, there is an ongoing fight about the actual number of deaths attributable to medical errors. I don’t have the time to read or get into that fight. So I’ll ask only one question: does it matter if the number is in the hundreds of thousands or merely tens of thousands? No, it doesn’t; medical errors need to be tackled head on, no matter how many people they kill. There will always be victims because doctors are humans and they make mistakes, like everybody else. But that doesn’t mean that they and their hospitals shouldn’t be held accountable. We, as patients, children and parents of patients, want that number to be as small as possible, is as simple as that. If the processes and methods of counting, assessing, and judging medical errors are kept hidden or worse, buried through misleading or downright false paperwork, then how can we trust the judgment of medical professionals? The authors’ letter to CDC attempts to do just that: by getting the hospitals to acknowledge medical errors on death certificates, the issue is becoming more visible. Where there is visibility and transparency, programs can then be implemented to reduce those numbers, whatever they may be.
Actually, the fact that the number of deaths attributable to medical error is disputable is a case in point; if there was a clear definition of what medical error is and a clear way of tracking it, then we would have a starting point on how to reduce its occurrence. And that’s why I will leave my picture where it is: to support the conversation around the need to better track medical error.
P.S.1 A newer paper, Stockwell et al. (2018) found that 10 % of the pediatric admissions in US hospitals end up with preventable adverse effects, most frequently as a result of hospital-acquired infections, followed by intravenous line complications, gastrointestinal harms, respiratory-related harms, and other causes (p. 4). The more worrisome fact is that this percentage is unchanged, at least between 2007 and 2012.
P.S.2 Just to make it clear, I will always go to doctors with an MD after their name, even if they make mistakes, because they give me and my loved ones the best chance of healing and survival. Calling out that there is more work to be done to improve our safety, particularity in the washing hands department (can’t believe this is still a thing!), doesn’t mean that I will go in the cuckoo land of homeopathy, chiropracty, and other “alternative” medicine.
REFERENCES:
Makary MA, & Daniel M. (3 May 2016). Medical error – the third leading cause of death in the US.BMJ, 353:i2139. doi: 10.1136/bmj.i2139, PMID: 27143499. ARTICLE | NPR cover
Joo S, Daniel M, Xu T, & Makary, MA (1 May 2016). RE: Methodology used for collecting national health statistics, Open Letter to U.S. Centers for Disease Control and PreventionFREE FULLTEXT PDF
I have begun this blogpost many times. I have erased it many times. That is because the subject of today – handwriting – is very sensitive for me. Most of what I wrote and subsequently erased was a rant: angry at rimes, full of profanity at other times. The rest were paragraphs that can be easily categorized as pleading, bargaining, imploring to teach handwriting in American schools. Or, if they already do, to do it less chaotically, more seriously, more consistently, with a LOT more practice and hopefully before the child hits puberty.
Because, contrary to most educators’ beliefs, handwriting is not the same as typing. Nor is printing / manuscript writing the same as cursive writing, but that’s another kettle.
Somehow, sometime, a huge disjointment happened between scholarly researchers and educators. In medicine, the findings of researchers tend to take 10-15 years until they start to be believed and implemented in medical practice. In education… it seems that even findings cemented by Nobel prizes 100 years ago are alien to the ranks of educators. It didn’t used to be like that. I don’t know when educators became distrustful of data and science. When exactly did they start to substitute evidence with “feels right” and “it’s our school’s philosophy”. When did they start using “research shows… ” every other sentence without being able to produce a single item, name, citation, paper, anything of said research. When did the educators become so… uneducated. I could write (and rant!) a lot about the subject of handwriting or about what exactly a Masters in Education teaches the educators. But I’m so tired of it before I even begun because I’m doing it for a while now and it’s exhausting. It takes an incredible amount of effort, at least for me, to bring the matter of writing so genteelly, tactfully, and non-threateningly to the attention of the fragile ego of the powers that be in charge of the education of the next generation. Yes, yes, there must be rarae aves among the educators who actually teach and do listen to or read papers on education from peer-reviewed journals; but I didn’t find them. I wonder who the research in education is for, if neither the educators nor policy makers have any clue about it…
Here is another piece of education research which will probably go unremarked by the ones it is intended for, i.e. educators and policy makers. Mueller & Oppenheimer (2014) took a closer look at the note-taking habits of 65 Princeton and 260 UCLA students. The students were instructed to take notes in their usual classroom style from 5 x >15 min long TED talks, which were “interesting but not common knowledge” (p. 1160). Afterwards, the subjects completed a hard working-memory task and answered factual and conceptual questions about the content of the “lectures”.
The students who took notes in writing (I’ll call them longhanders) performed significantly better at conceptual questions about the lecture content that the ones who typed on laptops (typers). The researchers noticed that the typers tend to write verbatim what it’s being said, whereas the longhanders don’t do that, which corresponds directly with their performance. In their words,
“laptop note takers’ tendency to transcribe lectures verbatim rather than processing information and reframing it in their own words is detrimental to learning.” (Abstract).
Because typing is faster than writing, the typers can afford to not think of what they type and be in a full scribe mode with the brain elsewhere and not listening to a single word of the lecture (believe me, I know, both as a student and as a University professor). Contrary to that, the longhanders cannot write verbatim and must process the information to extract what’s relevant. In the words of cognitive psychologists everywhere and present in every cognitive psychology textbook written over the last 70 years: depth of processing facilitates learning. Maybe that could be taught in a Masters of Education…
Pet peeves aside, the next step in the today’s paper was to see if you force the typers to forgo the verbatim note-taking and do some information processing might improve learning. It did not, presumably because “the instruction to not take verbatim notes was completely ineffective at reducing verbatim content (p = .97)” (p. 1163).
The laptop typers did take more notes though, by word count. So in the next study, the researchers asked the question “If allowed to study their notes, will the typers benefit from their more voluminous notes and show better performance?” This time the researchers made 4 x 7-min long lectures on bats, bread, vaccines, and respiration and tested them 1 week alter. The results? The longhanders who studied performed the best. The verbatim typers performed the worst, particularly on conceptual versus factual questions, despite having more notes.
For the sake of truth and in the spirit of the overall objectivity of this blog, I should note that the paper is not very well done. It has many errors, some of which were statistical and corrected in a Corrigendum, some of which are methodological and can be addressed by a bigger study with more carefully parsed out controls and more controlled conditions, or at least using the same stimuli across studies. Nevertheless, at least one finding is robust as it was replicated across all their studies:
“In three studies, we found that students who took notes on laptops performed worse on conceptual questions than students who took notes longhand” (Abstract)
Teachers, teach handwriting! No more “Of course we teach writing, just…, just not now, not today, not this year, not so soon, perhaps not until the child is a teenager, not this grade, not my responsibility, not required, not me…”.
REFERENCE: Mueller, PA & Oppenheimer, DM (2014). The Pen Is Mightier Than the Keyboard: Advantages of Longhand Over Laptop Note Taking. Psychological Science, 25(6): 1159–1168. DOI: 10.1177/0956797614524581. ARTICLE | FULLTEXT PDF | NPR cover
By Neuronicus, 1 Sept. 2019
P. S. Some of my followers pointed me to a new preregistered study that failed to replicate this paper (thanks, followers!). Urry et al. (2019) found that the typers have more words and take notes verbatim, just as Mueller & Oppenheimer (2014) found, but this did not benefit the typers, as there wasn’t any difference between conditions when it came to learning without study.
The authors did not address the notion that “depth of processing facilitates learning” though, a notion which is now theory because it has been replicated ad nauseam in hundreds of thousands of papers. Perhaps both papers can be reconciled if a third study were to parse out the attention component of the experiments by, perhaps, introspection questionnaires. What I mean is that the typers can do mindless transcription and there is no depth of processing, resulting in the Mueller & Oppenheimer (2014) observation or they can actually pay attention to what they type and then there is depth of processing, in which case we have Urry et al. (2019) findings. But the longhanders have no choice but to pay attention because they cannot write verbatim, so we’re back to square one, in my mind, that longhanders will do better overall. Handwriting your notes is the safer bet for retention then, because your attention component is not voluntary, but required for the task, as it were, at hand.
REFERENCE: Urry, H. L. (2019, February 9). Don’t Ditch the Laptop Just Yet: A Direct Replication of Mueller and Oppenheimer’s (2014) Study 1 Plus Mini-Meta-Analyses Across Similar Studies. PsyArXiv. doi:10.31234/osf.io/vqyw6. FREE FULLTEXT PDF
“We also find an interaction between total sneezes and initiator POA in rallies (table 1) indicating that the number of sneezes required to initiate a collective movement differed according to the dominance of individuals involved in the rally. Specifically, we found that the likelihood of rally success increases with the dominance of the initiator (i.e. for lower POA categories) with lower-ranking initiators requiring more sneezes in the rally for it to be successful (figure 2d). In fact, our raw data and the resultant model showed that rallies never failed when a dominant (POA1) individual initiated and there were at least three sneezes, whereas rallies initiated by lower ranking individuals required a minimum of 10 sneezes to achieve the same level of success. Together these data suggest that wild dogs use a specific vocalization (the sneeze) along with a variable quorum response mechanism in the decision-making process. […]. We found that sneezes, a previously undocumented unvoiced sound in the species, are positively correlated with the likelihood of rally success preceding group movements and may function as a voting mechanism to establish group consensus in an otherwise despotically driven social system.”
Intelligence is a dubious concept in psychology and biology because it is difficult to define. In any science, something has a workable definition when it is described by unique testable operations or observations. But “intelligence” had eluded that workable definition, having gone through multiple transformations in the past hundred years or so, perhaps more than any other psychological construct (except “mind”). Despite Binet’s first claim more than a century ago that there is such a thing as IQ and he has a way to test for it, many psychologists and, to a lesser extent, neuroscientists are still trying to figure out what it is. Neuroscientists to a lesser extent because once the field as a whole could not agree upon a good definition, it moved on to the things that they can agree upon, i.e. executive functions.
Of course, I generalize trends to entire disciplines and I shouldn’t; not all psychology has a problem with operationalizations and replicability, just as not all neuroscientists are paragons of clarity and good science. In fact, the intelligence research seems to be rather vibrant, judging by the publications number. Who knows, maybe the psychologists have reached a consensus about what the thing is. I haven’t truly kept up with the IQ research, partly because I think the tests used for assessing it are flawed (therefore you don’t know what exactly you are measuring) and tailored for a small segment of the population (Western society, culturally embedded, English language conceptualizations etc.) and partly because the circularity of definitions (e.g. How do I know you are highly intelligent? You scored well at IQ tests. What is IQ? What the IQ tests measure).
But the final nail in the coffin of intelligence research for me was a very popular definition of Legg & Hutter in 2007: intelligence is “the ability to achieve goals”. So the poor, sick, and unlucky are just dumb? I find this definition incredibly insulting to the sheer diversity within the human species. Also, this definition is blatantly discriminatory, particularly towards the poor, whose lack of options, access to good education or to a plain healthy meal puts a serious brake on goal achievement. Alternately, there are people who want for nothing, having been born in opulence and fame but whose intellectual prowess seems to be lacking, to put it mildly, and owe their “goal achievement” to an accident of birth or circumstance. The fact that this definition is so accepted for human research soured me on the entire field. But I’m hopeful that the researchers will abandon this definition more suited for computer programs than for human beings; after all, paradigmatic shifts happen all the time.
In contrast, executive functions are more clearly defined. The one I like the most is that given by Banich (2009): “the set of abilities required to effortfully guide behavior toward a goal”. Not to achieve a goal, but to work toward a goal. With effort. Big difference.
So what are those abilities? As I said in the previous post, there are three core executive functions: inhibition/control (both behavioral and cognitive), working memory (the ability to temporarily hold information active), and cognitive flexibility (the ability to think about and switch between two different concepts simultaneously). From these three core executive functions, higher-order executive functions are built, such as reasoning (critical thinking), problem solving (decision-making) and planning.
Now I might have left you with the impression that intelligence = executive functioning and that wouldn’t be true. There is a clear correspondence between executive functioning and intelligence, but it is not a perfect correspondence and many a paper (and a book or two) have been written to parse out what is which. For me, the most compelling argument that executive functions and whatever it is that the IQ tests measure are at least partly distinct is that brain lesions that affect one may not affect the other. It is beyond the scope of this blogpost to analyze the differences and similarities between intelligence and executive functions. But to clear up just a bit of the confusion I will say this broad statement: executive functions are the foundation of intelligence.
There is another qualm I have with the psychological research into intelligence: a big number of psychologists believe intelligence is a fixed value. In other words, you are born with a certain amount of it and that’s it. It may vary a bit, depending on your life experiences, either increasing or decreasing the IQ, but by and large you’re in the same ball-park number. In contrast, most neuroscientists believe all executive functions can be drastically improved with training. All of them.
After this much semi-coherent rambling, here is the actual crux of the post: intelligence can be trained too. Or I should say the IQ can be raised with training. Ritchie & Tucker-Drob (2018) performed a meta-analysis looking at over 600,000 healthy participants’ IQ and their education. They confirmed a previously known observation that people who score higher at IQ tests complete more years of education. But why? Is it because highly intelligent people like to learn or because longer education increases IQ? After carefully and statistically analyzing 42 studies on the subject, the authors conclude that the more educated you are, the more intelligent you become. How much more? About 1 to 5 IQ points per 1 additional year of education, to be precise. Moreover, this effect persists for a lifetime; the gain in intelligence does not diminish with the passage of time or after exiting school.
This is a good paper, its conclusions are statistically robust and consistent. Anybody can check it out as this article is an open access paper, meaning that not only the text but its entire raw data, methods, everything about it is free for everybody.
For me, the conclusion is inescapable: if you think that we, as a society, or you, as an individual, would benefit from having more intelligent people around you, then you should support free access to good education. Not exactly where you thought I was going with this, eh ;)?
Nota bene: I’d been asked what that “1 additional year” of education means. Is it with every year of education you gain up to 5 IQ points? No, not quite. Assuming I started as normal IQ, then I’d be… 26 years of education (not counting postdoc) multiplied by let’s say 3 IQ points, makes me 178. Not bad, not bad at all. :))). No, what the authors mean is that they had access to, among other datasets, a huge cohort dataset from Norway from the moment when they increased the compulsory education by 2 years. So the researchers could look at the IQ tests of the people before and after the policy change, which were administered to all males at the same age when they entered compulsory military service. They saw the increase in 1 to 5 IQ points per each extra 1 year of education.
An avid gamer myself, those who know me would hardly be surprised that I found a paper cheering StarCraft. A bit of an old game, but still a solid representative of the real-time strategy (RTS) genre.
About a decade ago, a series of papers emerged which showed that first-person shooters and action games in general improve various aspects of perceptual processing. It makes sense because in these games split second decisions and actions make the difference between win or lose, so the games act as training experience for increased sensitivity to cues that facilitate said decisions. But what about games where the overall strategy and micromanagement skills are a bit more important than the perceptual skills, a.k.a. RTS? Would these games improve the processes underlying strategical thinking in a changing environment?
Glass, Maddox, & Love (2013) sought to answer this question by asking a few dozen undergraduates with little gaming experience to play a slightly modified StarCraft game for 40 hours (1 hour per day). “StarCraft (published by Blizzard Entertainment, Inc. in 1998) (…) involves the creation, organization, and command of an army against an enemy army in a real-time map-based setting (…) while managing funds, resources, and information regarding the opponent ” (p. 2). The participants were all female because they couldn’t find enough male undergraduates that played computer games less than 2 hours per day. The control group had to play The Sims 2 for the same amount of time, a game where “participants controlled and developed a single ‘‘family household’’ in a virtual neighborhood” (p.3.). The researchers cleverly modified the StarCraft game in such a way that they replaced a perceptual component with a memory component (disabled some maps) and created two versions: one more complex (full-map, two friendly, two enemy bases) and one less so (half-map, one friendly, one enemy bases). The difficulty for all games was set at a win rate of 50%.
Before and after the game-playing, the subjects were asked to complete a huge battery of tests destined to test their memory and various other cognitive processes. By carefully parsing these out, the authors conclude that “forty hours of training within an RTS game that stresses rapid and simultaneous maintenance, assessment, and coordination between multiple information and action sources was sufficient” to improve cognitive flexibility. Moreover, authors point out that playing on a full-map with multiple allies and enemies is conducive to such improvement, whereas playing a less cognitive resources demanding game, despite similar difficulty levels, was not. Basically, the more stuff you have to juggle, the better your flexibility will be. Makes sense.
My favorite take from this paper though is not only that StarCraft is awesome, obviously, but that “cognitive flexibility is a trainable skill” (p. 5). Let me tell you why that is so grand.
Cognitive flexibility is an important concept in the neuroscience of executive functioning. The same year that this paper was published, Diamond was publishing an excellent review paper in which she neatly identified three core executive functions: inhibition/control (both behavioral and cognitive), working memory (the ability to temporarily hold information active), and cognitive flexibility (the ability to think about and switch between two different concepts simultaneously). From these three core executive functions, higher-order executive functions are built, such as reasoning (critical thinking), problem solving (decision-making) and planning.
Unlike some old views on the immutability of the inborn IQ, each one of the core and higher-order executive functions can be improved upon with training at any point in life and can suffer if something is not right in your life (stress, loneliness, sleep-deprived or sick). This paper adds to the growing body of evidence showing that executive functions can be trainable. Intelligence, however you want to define it, relies upon executive functions, at least some of them, and perhaps boosting cognitive flexibility might result in a slight increase in the IQ, methinks.
Bottom line: real-time strategy games with huge maps and tons of stuff to do are good for you. Here you go.
This is about naming things in science. You have been warned!
The DNA is made of four nucleobases: adenine (A), thymine (T), cytosine (C) and guanine (G). The “letters” of the code. Each of them has been named from where they were originally obtained by the scientists who first identified and/or isolated them.
Adenine was named thus because it was extracted from the pancreas of an ox, which is aden in Greek (the pancreas, not the ox), by the Nobel laureate Albrecht Kossel in 1885.
Thymine comes from thymic acid, which was extracted from the thymus gland of calves by the same Albrecht Kossel and Albert Neumann in 1893.
A year later, the duo named cytosine, another base obtained from the same thymus tissue. Cyto- pertains to cells in Greek.
Fifty years before that, Julion Bodo Unger, a German chemist, extracted the guanine from the guano of sea birds. Why was he looking at bird poop, curious minds inquire? Because he was studying it for its uses as fertilizer. The year of discovery was 1844 and the year of the naming was 1846.
And now you know…
REFERENCE: Unger, JB (1846). Bemerkungen zu obiger Notiz (Comments on the above notice), Annalen der Chemie und Pharmacie, 58: 18-20. From page 20: “ … desshalb möchte ich den Namen Guanin vorschlagen, welcher an seine Herkunft erinnert.” ( “… therefore I would like to suggest the name guanine, which is reminiscent of its origin”.) (Wikipedia translation). Google Books | Google Book PDF

















 REFERENCE: Callaway, E. (28 April 2020). The race for coronavirus vaccines: a graphical guide,
REFERENCE: Callaway, E. (28 April 2020). The race for coronavirus vaccines: a graphical guide, 










 Excerpt from Walker et al. (2017), p. 5:
Excerpt from Walker et al. (2017), p. 5: