I want to share an observation that’s been on my mind for a while. I was visiting a Zoo with my family before the vaccine was available for regular people, around early Spring 2021. A big Zoo. All the enclosures where animals were indoors (penguins, monkeys and so on) had a big sticker on the door asking to “Please wear a mask for our animals’ sake. They too can get COVID19”. An overwhelming majority were putting on their masks upon reading this sign. Really, close to 99% of people, adults and children alike. At the same zoo, the same people were entering maskless in the Gift Shop and other indoor facilities like toilets and so on. I eyeballed less than 10% were wearing masks in “human enclosures”. I spent a lot of time at this Zoo watching for this behavior instead of looking at the other animals to make sure I’m not imagining things.
My lesson: humans are not deemed worthy the masking trouble, but zoo animals are… Now please explain to me how no mask-wearing is about “freedom”, “COVID is a scam/flu/doesn’t exist”, “masks don’t work” and so on and not about a conscious moral choice to knowingly endanger other people and their kids?
By Neuronicus, 17 August 2021
EDIT: Mrs. Clinton’s first name is Hillary, not Hilary.
REFERENCES:
Howard J, Huang A, Li Z, Tufekci Z, Zdimal V, van der Westhuizen HM, von Delft A, Price A, Fridman L, Tang LH, Tang V, Watson GL, Bax CE, Shaikh R, Questier F, Hernandez D, Chu LF, Ramirez CM, Rimoin AW. (26 Jan 2021). An evidence review of face masks against COVID-19.Proceeding of the National Academy of Sciences of the USA, 118(4):e2014564118. doi: 10.1073/pnas.2014564118. PMID: 33431650. ARTICLE| FREE FULLTEXT PDFP.S. Since this paper was published, dozens of others have been published that say the same thing: wear a mask for all our sakes.
Some meme is circulating around saying that for any 1 dead of COVID-19 there is an x amount of people who survive but experience vastly debilitating and sometimes life long lasting diseases. That x number is usually a subject of controversy based on little or confusing hearsay-type of information. The believers in the x number use it to argue that mask-wearing and healthier behaviors literally save lives of people, while the non-believers in the x number, well… they just don’t believe the x number exists at all and that’s that. Either you die of COVID-19 or you survive and make a full recovery. I prefer to think that this is the case instead of the unfortunately way more probable, callous, cruel and dehumanizing “x exists and so what, I’m ok with people dying, ‘cause people die all the time, as long as it’s not me”.
The x number exists all right. Paterson et al. (2020) just published a paper last week (July 8th) that puts some numbers in the place of x, at least when it concerns neurological disorders. Because I have heard all sorts of “excuses” like, yeah, but those people who had it bad were old, had previous medical conditions, were black or poor or [insert your favorite post-hoc rationalization here], I decided to comb through the paper’s supplementals and give you a bit more of the background of the people investigated in this article.
If you’re not interested, you can skip the following section and go directly to the conclusion as long as you get the take-home message: many people of all sorts of ages and races, with no previous medical conditions and with mild COVID-19 symptoms can still have life long seriously debilitating neurological conditions. How many, you ask? I’m eyeballing almost a half of the investigated patients in this paper were not “at risk” in any way.
So. We have 43 patients treated from April 9 to May 15, 2020, in UK, out of which:
29 were SARS-CoV-2 PCR positive and definite, meaning a PCR test.
8 were probable meaning “clinical and laboratory features highly suggestive of COVID-19—lymphopenia, raised D-dimer, suggestive chest radiology in the absence of PCR evidence” p. 6
6 were possible in whom “temporal or laboratory features indicate an association but another cause was also found” p. 6
Demographics: 24 males and 19 females with ages ranging from 16–85 years, 53% were non-white.
Symptoms were classified as:
Mild (non-pneumonia or mild pneumonia)
Severe (dyspnoea and hypoxia requiring supplementary oxygen)
Both females and males, both whites and non-whites
Hospital admission reason: 6 neurological, 1 respiratory, 3 both
Past medical history : 4 none, 3 hypertension, 2 cancer, 1 stroke, 2 diabetes, 1 asthma
Days of onset of encephalopathies from onset of COVID-19 symptoms: -4 to 21
Severity of COVID-19 symptoms: 6 mild, 2 severe, 2 critical
Diagnosis: 8 definite, 2 probable COVID-19
Recovery: 7 complete, 1 incomplete, 1 significant, 1 not recovered.
Survival: all 10 are alive
Vignette A: As a note for people who think a bit of delirium is not a big deal, let’s peak at a case that the authors describe in the paper for representative reasons. A 55-year old White woman with no previous medical or psychiatric conditions was admitted to hospital with mild to severe COVID-19 symptoms and a positive SARS-CoV2 test. She stayed in the hospital for 3 days, requiring minimal oxygen. But after discharge, the woman started behaving oddly, confused, agitated, putting on and off her coat repeatedly, hallucinated lions and monkeys in the house, other auditory hallucinations, had persecutory delusion, Capgras delusion (husband replaced by impostor), and became aggressive and combative with family and hospital staff. This started 17 days after her fist COVID-19 symptoms which were fever, cough, aches and loss of smell and taste. Normal brain MRI and EEG. She was put on serious antipsychotics with an on-off improvement result. She’s classified as significantly recovered.
12 patients had neuroinflammatory syndromes (encephalitis) post-COVID
Age: 27-60
Hospital admission reason: 6 neurological, 1 respiratory, 3 both
Both females and males, both whites and non-whites
Days of onset of syndrome from onset of COVID-19 symptoms: -6 to 27
Severity of COVID-19 symptoms: 6 mild, 2 severe, 2 critical
Diagnosis: 8 definite, 3 probable, 1 possible
Past medical history: 3 none, 3 diabetes, 2 asthma, 3 hypertension, 2 arthritis, 1 hypothyroidism, 1 treated breast cancer with high cholesterol and other diseases and this is the one who died.
Severity of COVID-19 symptoms: 6 mild, 2 severe, 4 critical
Recovery: 1 complete, 10 incomplete, 1 died
Survival: 11 alive, 1 dead (which had mild symptoms)
Vignette B: A 65-year-old Black female with osteoarthritis and a 2-year history of cognitive decline was admitted for involuntary right hand and then widespread involuntary movements. Then she developed complex visual hallucinations (people in the house, objects flying in the room), vision impairments including double vision, speaking impairments, disorientation and confusion, shaking, remarkable twitching and hyper reflexes. “MRI brain, EEG and CSF examination were normal” p. 12. She had a positive SARS-CoV2 test and severe COVID-19 symptoms, meaning she required oxygen therapy. Given medicines for muscle spasms and oxygen for COVID-19. She’s classified as incomplete recovery.
Vignette C: A 52-year-old Asian male with asthma presented with 10 days of cough, difficulty breathing and muscle aches. The SARS-CoV2 test was positive. His oxygen supply was getting worse and he required intubation for 17 days, meaning now his symptoms are considered critical. He was slow to wake up from intubation. MRI showed significant lesions and cysts with white matter damage and haemorrhage. He has a severely impaired conscious level responding to pain only. He’s classified as incomplete recovery.
Vignette D: A 47 year old female of Other ethnicity with asthma as a previous medical condition presented neurological symptoms: left side numbness and weakness, with headache, vomiting and reduced conscious level. Prior to this, for a week she had cough, fever and shortness of breath. All other markers and symptoms (minus neurological) pointed to COVID-19 but no PCR test was administered. Because she had low conscious level she was incubated, thus her COVID-19 symptoms are catalogued as severe, even if the reason of intubation was not low oxygen. MRI showed severe brain and brain blood vessels swelling. Was aggressively treated for brain swelling. After 2 days of this treatment when she was not responding and when she developed fixed dilated right pupil, emergency surgery was performed to remove part of her skull to release intracranial pressure from all the swelling. After 4 more days of intubation she was de-intubated and “continues to improve clinically, and is able to weight bear with support” p. 10. She’s classified as incomplete recovery.
Vignette E: A 52 year-old White male with no past medical history presented with progressive limb weakness, headache, vomiting, and back pain that lasted for the past 3 days. MRI showed multiple lesions in the brain. Over 5 days, these lesions increased in size and there were multiple bleeding sites in the brain. He was positive for SARS-CoV2 and 3 days later developed fever and shortness of breath. About the same time his neurological symptoms increased in severity and number. A nerve conduction test supported a diagnosis of Guillain–Barré syndrome (a nasty autoimmune disease in which your immune system eats your nerves). He was intubated due to oxygen requirements. Three days after corticosteroid treatment he was able to open eyes and mouth words and after 2 weeks, he was able to talk and flex both arms. He’s classified as incomplete recovery. He’s still in the hospital.
8 patients had strokes post-COVID
Age: 24 -85
Both females and males, both whites and non-whites.
Days of onset of syndrome from onset of COVID-19 symptoms: -2 to 15.
Severity of COVID-19 symptoms: 6 mild, 2 severe, 2 critical
Diagnosis: 6 definite, 2 probable
Reason for hospital admission: 5 neurological, 3 respiratory
Past medical history: 2 none, 2 with hypertension, 1 with stroke, 1 obese, 2 heart disease (1 of them is the one who died) and others
Severity of COVID-19 symptoms: 5 mild, 3 severe
Recovery: 1 complete, 3 incomplete, 1 no improvement (3 still in the hospital)
Survival: 7 alive, 1 dead (of the ones with severe symptoms)
Vignette F: A 58-year-old Black male with only arthritis of the spine as a pre-existing condition came to the hospital with difficulty in speaking and weakness on the right side after 2 days of coughing and being tired. He had a high-risk occupation for getting COVID-19 and all other COVID-19 signs and symptoms were there minus a COVID-19 test. So he is thought to be probably carrying it. Brain CT showed a stroke. Treated with heparin for a lung blood clot and other anti-blood clot medicines for the stroke. On day 8 he was discharged to the Rehabilitation unit of the hospital.
7 patients developed Guillain–Barré syndrome (GBS) post-COVID
Age: 20-63
All males, both whites and non-whites.
Days of onset of syndrome from onset of COVID-19 symptoms: -1 to 21.
Severity of COVID-19 symptoms: 6 mild, 2 severe, 2 critical
Diagnosis: 4 definite, 4 possible
Reason for hospital admission: all neurological
Past medical history: 4 none, 1 with stroke and myeloma, 1 with high cholesterol, and 1 with diabetes, headaches and arrhythmia
Severity of COVID-19 symptoms: 7 mild, 1 severe
After treatment with immunoglobulins: 1 requires assisted ventilation, 1 is bedridden, 5 able to walk 5m but incapable of manual work/running, and 1 unknown
Survival: all
5 patients developed neurological symptoms difficult to characterizepost-COVID
Age: 16-40
Both males and females, both whites and non-whites.
Days of onset of syndrome from onset of COVID-19 symptoms: 6 to 26.
Severity of COVID-19 symptoms: 2 mild, 1 severe, 2 critical
Diagnosis: 3 definite, 1 probable, 1 possible
Reason for hospital admission: 2 neurological, 2 respiratory, 1 other
Past medical history: 1 none, 1 heavy periods, 1 with epilepsy, hypertension, congenital disorders and all sorts of other stuff, 1 with leukemia, and 1 with inflammation of the eyes and joints
Severity of COVID-19 symptoms: 7 mild, 1 severe
Recovery: 1 complete, 3 incomplete , and 1 no improvement (3 still in the hospital)
Survival: 7 alive, 1 dead (of the ones with severe symptoms)
These patients’ symptoms ranged from the headaches to seizures, from weakness to low conscious level. Some also had hemorrhages, encephalopathy, brain abscess, diarrhea, cardiac stuff, all sorts. MRIs were all abnormal except for the one who was declared recovered and discharged.
CONCLUSIONS
To recapitulate, what I did was basically re-write the paper’s tables in lay terms because few of us are proficient in medical jargon, but, more importantly, even fewer – except the scientists and medical doctors – have the time and patience to comb through the supplemental to form the image I gave you. So here you go. Professionals don’t need my blog, they can go directly to the bottom of the post and read the source in original. The image I wanted to convey is that
By long lasting I mean “irreversible”, even if slowly improvable. Please note that the vast majority of these patients were admitted to the hospital not for COVID-19 respiratory symptoms, but for neurological symptoms.
There’s also something else of extraordinary interest in the paper. Eight of the patients had either brain biopsies or spinal tap tested for SARS-CoV2 and all these tests were negative, meaning the virus is not itself causing these neurological problems. In some patients, there was evidence of the cytokine storm, meaning the virus put the immune system in overdrive and this one, in turn, attacked the body, here the brain. So far, the autoimmune hypothesis seems to be the most plausible and parsimonious explanation.
As far the x number is concerned, the authors just gave us the data and let us interpret it. They do offer a hint of just how to interpret them though: the number of brain inflammation cases they saw in 5-weeks is normally seen in London only over a period of 5 months (p. 14). You do the math.
Also, some commentator on the Facebook post raised the question of asymptomatics. Which is a very good question. How do they fare? I don’t know and neither are you. But let me remind you that most of the people in this study were admitted to hospital for neurological reasons, not COVID-19 symptoms. So if they were never having the COVID-19 symptoms, i.e. were asymptomatics, nobody would have done a COVID-19 test on them… and so they’d be treated as regular neurological patients. To figure out what happens to the asymptomatics we need to wait probably a year when we can look at the general epidemiological incidence of heart attacks or GBS or strokes in the general population. And so we’ll probably attribute that increase to COVID-19.
REFERENCE: Paterson RW, Brown RL, Benjamin L, Nortley R, Wiethoff S, Bharucha T, Jayaseelan DL, Kumar G, Raftopoulos RE, Zambreanu L, Vivekanandam V, Khoo A, Geraldes R, Chinthapalli K, Boyd E, Tuzlali H, Price G, Christofi G, Morrow J, McNamara P, McLoughlin B, Lim ST, Mehta PR, Levee V, Keddie S, Yong W, Trip SA, Foulkes AJM, Hotton G, Miller TD, Everitt AD, Carswell C, Davies NWS, Yoong M, Attwell D, Sreedharan J, Silber E, Schott JM, Chandratheva A, Perry RJ, Simister R, Checkley A, Longley N, Farmer SF, Carletti F, Houlihan C, Thom M, Lunn MP, Spillane J, Howard R, Vincent A, Werring DJ, Hoskote C, Jäger HR, Manji H, Zandi MS; UCL Queen Square National Hospital for Neurology and Neurosurgery COVID-19 Study Group (8 Jul 2020). The emerging spectrum of COVID-19 neurology: clinical, radiological and laboratory findings, Brain, online ahead of print PMID: 32637987. DOI: 10.1093/brain/awaa240ARTICLE | FREE FULLTEXT PDF | SUPPLEMENTALS | Deutsche Welle cover | University College London Press release
There is hope for a vaccine. Serious hope. It will take probably 12 to 18 months until we have it. Maybe a little bit longer. But it looks like we will have it. Just continue your physical distancing, wear masks, be considerate to your fellow humans and it’ll be alright. We’ll bounce back and because we – the people – make up this extraordinary concept of economy, so shall it. After this pandemic will pass, hopefully we will not return to normal; instead, we will emerge a bit wiser, a bit more careful, a bit more compassionate. Meanwhile, throw some grateful words to your nearest scientist, whether or not they work on COVID-19.
REFERENCE: Callaway, E. (28 April 2020). The race for coronavirus vaccines: a graphical guide,Nature, 580: 576-577 (2020). doi: 10.1038/d41586-020-0121-y. FREE FULLTEXT PDF
In the past few days, a new hot subject has gripped the attention of various media and concerned the medical doctors, as if they don’t have enough to deal with: chloroquine. That is because the President of the U.S.A., Donald Trump, endorsed chloroquine as treatment of COVID-19, a “game changer”, despite his very own director of the National Institute of Allergy and Infectious Diseases (NIAID), Dr. Anthony Fauci, very emphatically and vehemently denying that the promise of (hydroxy)chloroquine is beyond anecdotal (see the White House briefing transcript here).
Many medical doctors spoke out urging caution against the drug, particularly against the combination the President endorses: hydroxychloroquine + azithromycin. As I understand it, this combo can be lethal as it can lead to fatal arrhythmia.
As for the (hydroxy)cloroquine’s possibility to help treat COVID-19, the jury is still out. Far out. Meaning that there have been a few interesting observations of the drugs working in a Petri dish (Liu et al. 2020, Wang et al., 2020), but as any pharma company knows, there is a long and perilous way from Petri dishes to pharmacies. To be precise, only 1 in 5000 drugs get from pre-clinical trials to approval and it takes about 12 years for this process to be completed (Kaljevic et al., 2004). The time is so long not because red tape, as some would deplore, but because it takes time to see what it does in humans (Phase 0), what doses are safe and don’t kill you (Phase 1), does it work at all for the intended disease (Phase 2), compare it with other drugs and evaluate the long-term side effects (Phase 3) and, finally, to see the risks and benefits of this drug (Phase 4). While we could probably get rid of Phase 0 and 4 when there is such a pandemic, there is no way I would submit my family to anything that hasn’t passed phases 1, 2, and 3. And those take years. With all the money that a nation-state has, it would still take 18 months to do it semi-properly.
Luckily for all of us, chloroquine is a very old and established anti-malarial medicine, and as such we can safely dispense of Phases 0, 1, and 4, which is fine. So we can start Phase 2 with (hydroxy)chloroquine. And that is exactly what WHO and several others are doing right now. But we don’t have enough data. We haven’t done it yet. So one can hope as much as they want, but that doesn’t make it faster.
Unfortunately – and here we go to the crux of the post -, following the President’s endorsement, many started to hoard chloroquine. Particularly the rich who can afford to “convince” an MD to write them a script for it. In countries where chloroquine is sold without prescription, like Nigeria, where it is used for arthritis, people rushed to clear the pharmacies and some didn’t just stockpiled it, but they took it without reason and without knowing the dosage. And they died. [EDIT, 23 March 2020. If you think that wouldn’t ever happen in the land of the brave, think again, as the first death to irresponsible taking chloroquine just happened in the USA]. In addition, the chloroquine hoarding in US by those who can afford it (is about $200 for 50 pills) lead to lack of supply for those who really need it, like lupus or rheumatology patients.
For those who blindly hoard or take chloroquine without prescription, I have a little morsel of knowledge to impart. Remember I am not an MD; I hold a PhD in neuroscience. So I’ll tell you what my field knows about chloroquine.
Both chloroquine and hydroxychloroquine can cause severe psychosis.
That’s right. More than 7.1 % of people who took chloroquine as prophylaxis or for treatment of malaria developed “mental and neurological manifestations” (Bitta et al., 2017). “Hydroxychloroquine was associated with the highest prevalence of mental neurological manifestations” (p. 12). The phenomenon is well-reported, actually having its own syndrome name: “chloroquine-induced psychosis”. It was observed more than 50 years ago, in 1962 (Mustakallio et al., 1962). The mechanisms are unclear, with several hypotheses being put forward, like the drugs disrupting the NMDA transmission, calcium homeostasis, vacuole exocytosis or some other mysterious immune or transport-related mechanism. Because the symptoms are so acute, so persistent and so diverse than more than one brain neurotransmitter system must be affected.
Chloroquine-induced psychosis has sudden onset, within 1-2 days of ingestion. The syndrome presents with paranoid ideation, persecutory delusions, hallucinations, fear, confusion, delirium, altered mood, personality changes, irritability, insomnia, suicidal ideation, and violence (Biswas et al., 2014, Mascolo et al., 2018). All these at moderately low or therapeutically recommended doses (Good et al., 1982). One or two pills can be lethal in toddlers (Smith & Klein-Schwartz, 2005). The symptoms persist long after the drug ingestion has stopped (Maxwell et al., 2015).
Still want to take it “just in case”?
P.S. A clarification: the chemical difference between hydroxychloroquine and chloroquine is only one hydroxyl group (OH). Both are antimalarial and both have been tested in vitro for COVID-19. There are slight differences between them in terms of toxicity, safety and even mechanisms, but for the intents of this post I have treated them as one drug, since both produce psychosis.
REFERENCES:
1) Biswas PS, Sen D, & Majumdar R. (2014, Epub 28 Nov 2013). Psychosis following chloroquine ingestion: a 10-year comparative study from a malaria-hyperendemic district of India.General Hospital Psychiatry, 36(2): 181–186. doi: 10.1016/j.genhosppsych.2013.07.012, PMID: 24290896 ARTICLE
2) Bitta MA, Kariuki SM, Mwita C, Gwer S, Mwai L, & Newton CRJC (2 Jun 2017). Antimalarial drugs and the prevalence of mental and neurological manifestations: A systematic review and meta-analysis. Version 2. Wellcome Open Research, 2(13): 1-20. PMCID: PMC5473418, PMID: 28630942, doi: 10.12688/wellcomeopenres.10658.2 ARTICLE|FREE FULLTEXT PDF
4) Good MI & Shader RI. Lethality and behavioral side effects of chloroquine (1982). Journal of Clinical Psychopharmacology, 2(1): 40–47. doi: 10.1097/00004714-198202000-00005, PMID: 7040501.ARTICLE
3) Kraljevic S, Stambrook PJ, & Pavelic K (Sep 2004). Accelerating drug discovery. EMBO Reports, 5(9): 837–842. doi: 10.1038/sj.embor.7400236, PMID: 15470377, PMCID: PMC1299137. ARTICLE| FREE FULLTEXT PDF
4) Mascolo A, Berrino PM, Gareri P, Castagna A, Capuano A, Manzo C, & Berrino L. (Oct 2018, Epub 9 Jun 2018). Neuropsychiatric clinical manifestations in elderly patients treated with hydroxychloroquine: a review article. Inflammopharmacology, 26(5): 1141-1149. doi: 10.1007/s10787-018-0498-5, PMID: 29948492. ARTICLE
5) Maxwell NM, Nevin RL, Stahl S, Block J, Shugarts S, Wu AH, Dominy S, Solano-Blanco MA, Kappelman-Culver S, Lee-Messer C, Maldonado J, & Maxwell AJ (Jun 2015, Epub 9 Apr 2015). Prolonged neuropsychiatric effects following management of chloroquine intoxication with psychotropic polypharmacy.Clinical Case Reports, 3(6): 379-87. doi: 10.1002/ccr3.238, PMID: 26185633. ARTICLE | FREE FULLTEXT PDF
6) Mustakallio KK, Putkonen T, & Pihkanen TA (1962 Dec 29). Chloroquine psychosis?Lancet, 2(7270): 1387-1388. doi: 10.1016/s0140-6736(62)91067-x, PMID: 13936884. ARTICLE
7) Smith ER & Klein-Schwartz WJ (May 2005). Are 1-2 dangerous? Chloroquine and hydroxychloroquine exposure in toddlers.The Journal of Emergency Medicine, 28(4): 437-443. doi: 10.1016/j.jemermed.2004.12.011, PMID: 15837026. ARTICLE
Studies about chloroquine and hydoxychloroquine on SARS-Cov2 in vitro:
Liu, J., Cao, R., Xu, M., Wang, X., Zhang, H., Li, Y., Hu, Z., Zhong, W., & Wang, M. (18 March 2020). Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discovery, 6 (16), https://doi.org/10.1038/s41421-020-0156-0ARTICLE | FREE FULLTEXT PDF
Wang, M., Cao, R., Zhang, H., Yang, X., Liu, J., Xu, M., Shi, Z., Hu, Z., Zhong, W., & Xiao, G. (18 March 2020). Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Research, 30: 269–271. https://doi.org/10.1038/s41422-020-0282-0.ARTICLE | FREE FULLTEXT PDF
First study about chloroquine and hydoxychloroquine on SARS-Cov2 in vivo below. Unfortunately, it has some methodological flaws, see here and here, which hopefully will be corrected once the peer-reviewers will take a closer look at it. UPDATE [31-3-2020]: It seems the article is flawed in more than one way, with serious ethical issues (timeline of treatment doesn’t match the methods reported, patients appear and disappear from data points, graphs different depending on the venue, published in the same journal where the author is editor, no peer-review, no blind, no placebo, controls barely tested, plus, no reputable researcher should announce that they are the genius that cured COVID-19 on a YouTube video, particularly when they get to publish in 24 hours anyway).
Anyway, here it is:
Gautret P, Lagier J-C, Parola P, Hoang VT, Meddeb L, Mailhe M, Doudier B, Courjon J, Giordanengo V, Esteves Vieira V, Tissot Dupont H,Colson SEP, Chabriere E, La Scola B, Rolain J-M, Brouqui P, Raoult D. (20 March 2020). Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. International Journal of Antimicrobial Agents, PII:S0924-8579(20)30099-6, https://doi.org/10.1016/j.ijantimicag.2020.105949. ARTICLE | FREE FULLTEXT PDF
These studies are also not peer reviewed or at the very least not properly peer reviewed. I say that so as to take them with a grain of salt. Not to criticize in the slightest. Because I do commend the speed with which these were done and published given the pandemic. Bravo to all the authors involved (except maybe the last one f it proves to be fraudulent). And also a thumbs up to the journals which made the data freely available in record time. Unfortunately, from these papers to a treatment we still have a long way to go.
I was looking for what kills coronaviruses and I found this little gem in a paper by Walker & Ko (2007):
“MHV coronavirus was easily inactivated in PBS with 0.01% Tween but was relatively stable when suspended in MEM with 10% FBS”.
Tween is a relatively inexpensive standard molecular biology reagent for cell culture. Is otherwise known as POE (20) sorbitan monooleate, Polyethylene glycol sorbitan monooleate, Polyoxyethylenesorbitan monooleate, Polysorbate 80, Sigma says. It costs about $30 for 100 ml, but you could probably get it cheaper if bought in bulk, like I did a few months ago.
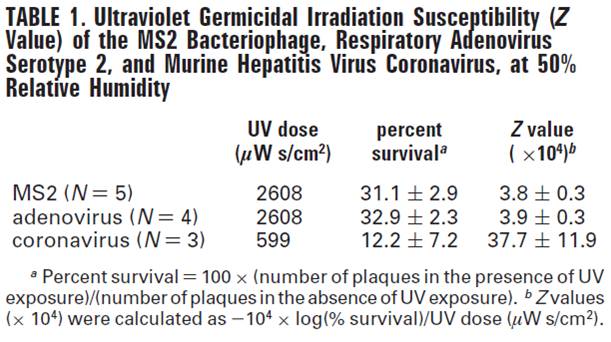
The paper in itself is on a different subject: comparing survival rate of the infectious agents after exposure to UV light. The one sentence about Tween was put in to emphasize differences between the infectious agents. The actual point of the paper is that while the bacteriophage MS2 and the respiratory adenovirus serotype 2 were not affected too much by UV, the murine hepatitis coronavirus was. Namely, after exposure to a dose of 599 microW s/cm2 of 254 nm UV, the coronavirus survival was only 12.2 % +/- 7.2, but to reduce the MS2 and adenovirus survival rate to around 32%, a much higher dose of UV of 2608 microW s/cm2 was needed (see Table).
From Walker & Ko (2007).
The infectious agents were aerosolized. This is important because the “UV susceptibility is higher in viral aerosols than in viral liquid suspensions” (p. 5464).
Of extreme importance: DO NOT SHINE UV ON SKIN! It will harm you more than it will harm the virus:
The only thing I’m a bit unclear is the duration of UV exposure. In the Methods it says: “16.2 s at 12.5 L/min airflow […] was considered the UV exposure time” (p. 5461), but elsewhere in the paper we find: “The duration of sample collection was 15 min, with the UV on (UV dose = 2608 or 599 microWs/cm2) or off” (p. 5462). So weren’t the aerosols exposed for 15 minutes then? Or they passed away since there was an airflow in the experimental chamber and then they were only exposed for 16 sec? I dunno, it’s not my field.
Nor is cell culture my field, so I’m definitely not an expert though I have learned how to do it as a matter of principle because it keeps happening around me and in the papers I read. So perhaps the fact that Tween kills coronaviruses might be common knowledge for a good portion of the molecular biologists and immunologists, but maybe not for everybody. So here you go:
P.S. As soon as I published, I have been thoroughly (and repeatedly!) informed that every scientist that works with viruses knows that Tween kills coronaviruses. Because… drum roll… Tween is a soap. Duh! And we know how soap kills viruses, by dissolving their protective cover. Oh well :). I’d rather be chided for repeating well-known facts than for spreading disinformation.
REFERENCE: Walker, C. M., & Ko, G. (1 Aug 2007). Effect of Ultraviolet Germicidal Irradiation on Viral Aerosols. Environmental Science & Technology, 41(15), 5460–5465. PMID: 17822117, DOI: 10.1021/es070056uARTICLE






 REFERENCE: Callaway, E. (28 April 2020). The race for coronavirus vaccines: a graphical guide,
REFERENCE: Callaway, E. (28 April 2020). The race for coronavirus vaccines: a graphical guide,